

Hi there ! I’m Mao who works for Home Nursing Station.
Assessment is the analysis and evaluation of patient information.
The basic idea of assessment is to consider what is happening in the patient’s body and how it will change in the next.
Assessment is an important item for Home Nursing, so I hope you understand it well.
I will also introduce how to actually use the assessment sheet.
If you immediately need an assessment sheet written by Japanese and English, please go to link below.
If you are interested in Home Nursing, please refer to related links.

What’s Assessment ?

Assessment is the way evaluating the patient’s condition from objective measurement data.
The assessment can be broadly categorized as shown in the figure below.
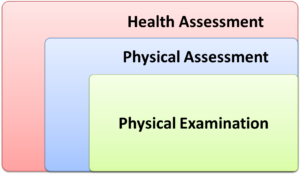
Assessment can be divided into “Health Assessment” that evaluates physical and psychological conditions, “Physical Assessment” that evaluates only physical conditions, and “Physical Examination” that involves interviews and palpation.
The main purpose of assessment is to determine which stage the patient is in and to make necessary care clearly.
Assessment for Home Nursing
In case of Home Nursing, general idea of assessment is basically based on the same concept.
However, since Home Nursing is care provided at the patient’s home, it is important to be able to provide services that meet the demands of the patient and their families.
The contents of the basic services are written in the “Home Nursing Instructions” created by the doctor, but actual care is provided by nurse with more closely providing services to the patient and family than hospital.
Home Nursing cannot be said by only manual and textbook.
Important Points for Assessment

The word “Assessment” has a meaning of “Evaluation”.
For evaluating the patient, I will explain couple of points.
1, Repeat the assessment
2, Do not have a preconceptions
3, Be aware the discomfort
4, Know the assessment is a tool
I will explain the each point one by one.
Repeat the assessment
Mainly the nurse will visit patient’s home once or twice a week.
Since the patient’s physical condition changes on a daily basis, it is important to repeatedly check an assessments so that the latest information can be obtained.
Also, patients’ feelings and needs change, so be sure to collect information so that you can answer their needs.
Do not have a preconceptions
Experienced nurses who have worked for long time as nurse may have preconceived idea.
No matter how experienced you are, do not have preconceived notions. Just listen to the opinions of care managers and helpers for assessments.
Be aware the discomfort
The important thing in the assessment is to notice the sense of incongruity, such as “unusual” or “something strange”.
In this blog, I always say, “Make a decision based on objective information” when measuring vital signs, but it is also important to value the discomfort that you notice.
By interacting with patients on a daily basis, you will become aware of the patient’s condition, which cannot be expressed in data or numbers.
Know the assessment is a tool
Assessment is a means, not an end.
Even if the assessment is perfect, it does not mean that you can provide perfect care.
Remember, it’s the nurses who actually take care of patients, so it’s just as important to develop the skills to do so.
Our purpose as a nurse is that to meet a patient’s demands.
Tip for Assessment

I will more explain about tip for assessment.
1, Grasping the normal conditions for notice abnormality
2, Check if assessment is properly done
3, Others see your assessment sheet
Grasping the normal conditions for notice abnormality
In order to understand the patient’s abnormalities, it is necessary to first recognize the normal condition on a daily basis.
The most important thing is to understand the normal state in order to judge whether it is “Normal” or “Abnormal” when a problem occurs even in our daily lives.
In short, it is precisely because we know the normal state that we can judge whether it is abnormal or not.
Check if assessment is properly done
Ideally, the results of an assessment should be the same regardless of who conducts it.
That being said, different nurses use slightly different expressions, I recommend that you need a check with your seniors and superiors to see if you have done the assessment correctly.
It is also an effective method to have not only nurses but also care managers and helpers confirm and receive multifaceted opinions.
Getting a variety of opinions will greatly improve the accuracy of your assessment.
Others see your assessment sheet
Assessment is just “Information”.
Information such as the patient’s condition must be written in a way that everyone can understand easily.
Be aware that the assessment information you write will be shared with other nurses, Doctor, Care Manager and such as Home Nursing Stations as well.
How to Use Assessment Sheet

From here, I will explain what is actually written on the assessment sheet and tips on how to use it.
The assessment sheet is a brief description of the patient’s basic information, physical and mental condition, and what kind of care is needed.
Many stations have a fixed assessment format, so the nurse mainly fills in the sheet.
What’s Written in Assessment Sheet ?
Common assessment sheet is written as following information.
・Patient’s name, address, date of birth, etc.
・Family structure
・Nursing care level
・Health recipient information
・Usage status of medical institutions, etc.
・Lifestyle habits, etc.
・Usage status of medical services
・Requests of the individual or family members, etc.
– Housing information (toilet and bathroom facilities, etc.)
・Medical history and current symptoms
・Height and weight
・Opinion letter from attending physician
・ADL/IADL (Activities of Daily Living / Instrument Activities of Daily Living)
・The state of urine and feces
・Cognitive level and communication method
・Social activities, etc.
・Other matters
There are many items, but based on these contents, care managers and doctors judge the necessary care menu, etc., then care is assigned to nurses.
Of cause care menu is also determined by consideration of wishes of the patient and his/her family too.
Assessment Sheet Format
I know the assessment sheet is available at the Home Nursing Stations to which you belong, so fill it out according to the format.
For reference, you can find 5 assessment sheets quoted from the site “『ヘルパー会議室』(Helper Meeting Room)”.
If you register for free, you can download the assessment sheet.
However in order those format are written in Japanese, I make them with multi languages of Japanese and English below.
Download the free assessment sheet here.

Made by “『ヘルパー会議室』Helper Meeting”
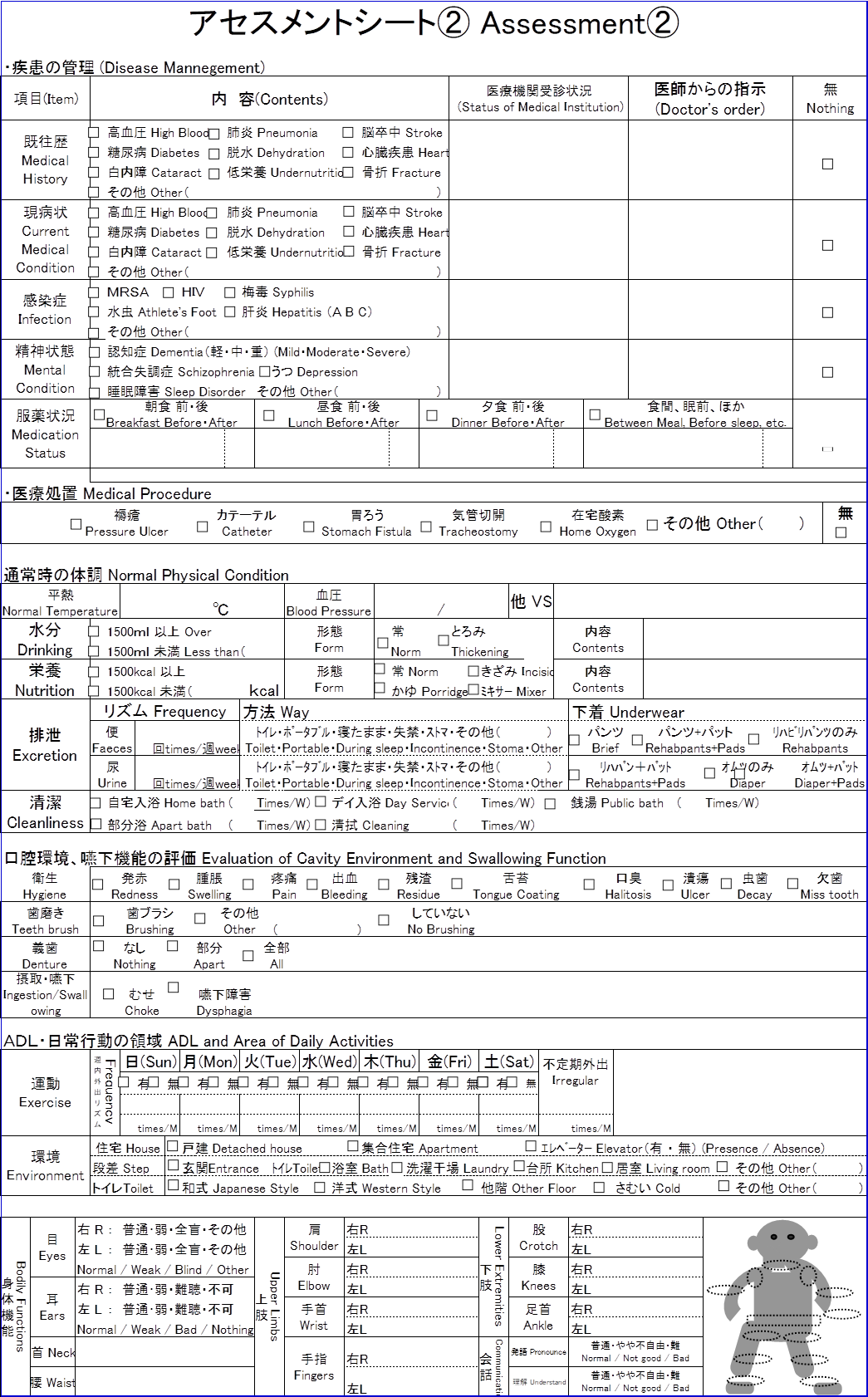
Made by “『ヘルパー会議室』Helper Meeting”
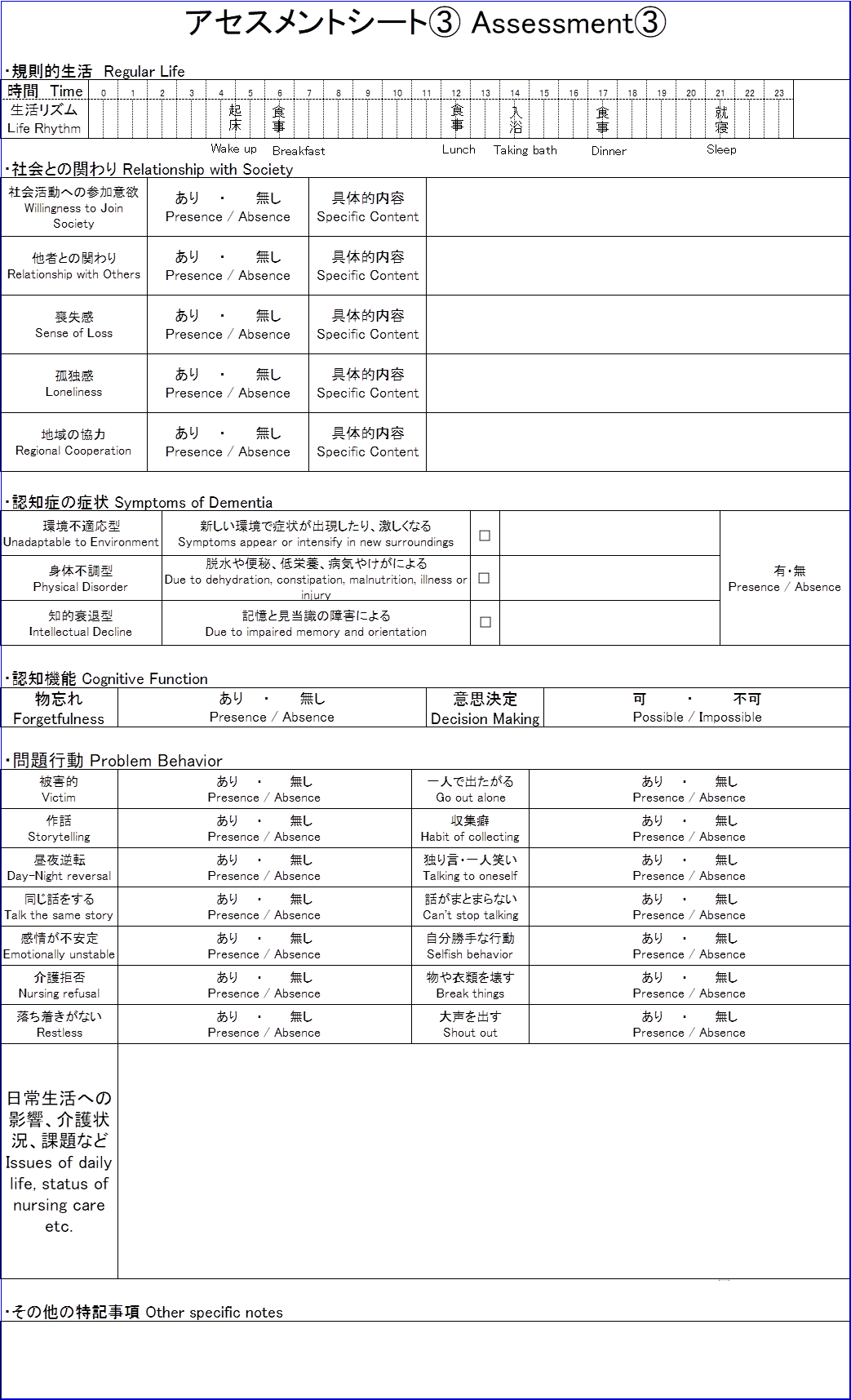
Made by “『ヘルパー会議室』Helper Meeting”
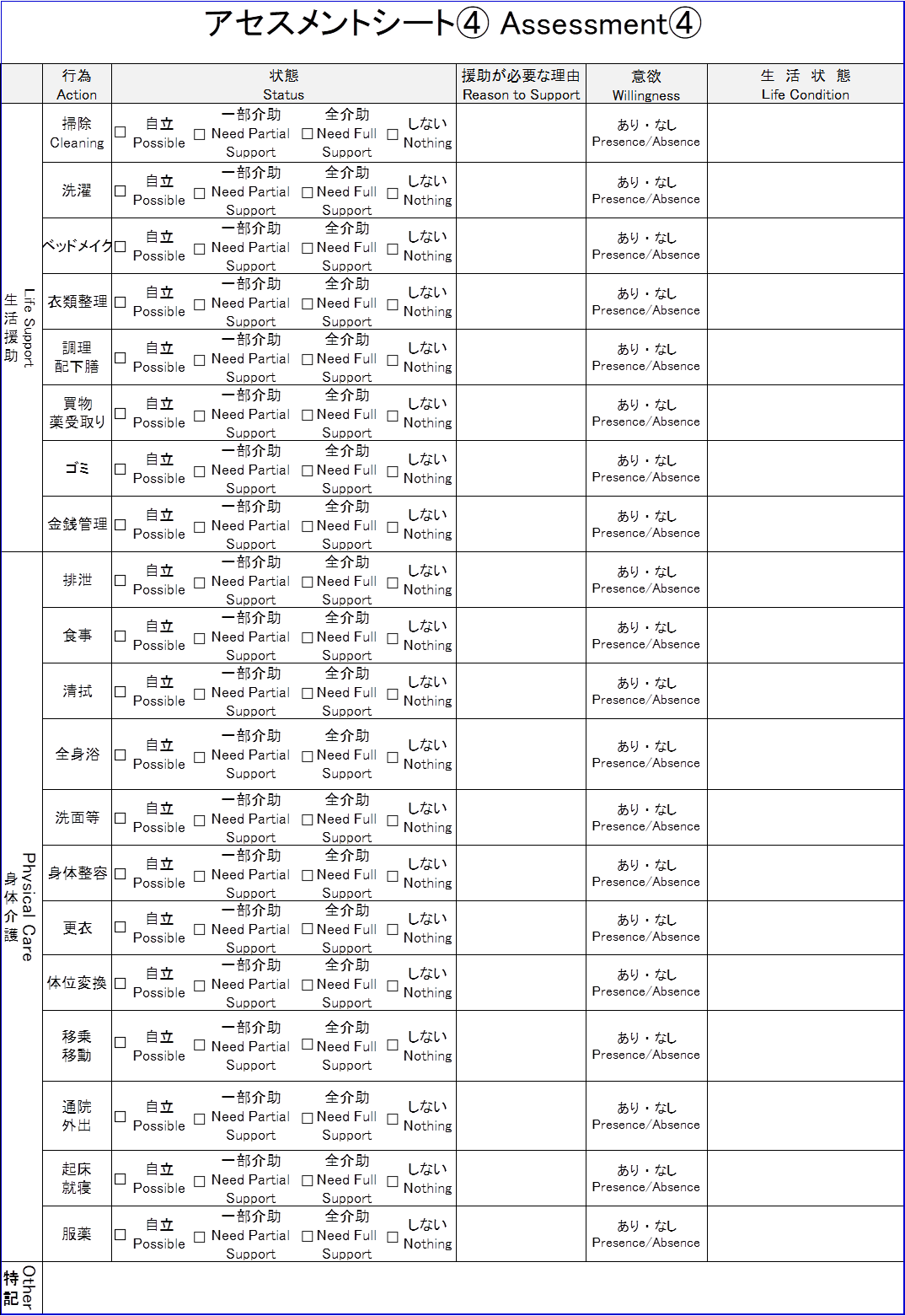
Made by “『ヘルパー会議室』Helper Meeting”

Made by “『ヘルパー会議室』Helper Meeting”
You can download each formats from here.
Propose by using “SBAR” in Emergency
I hope you understood that the assessment sheet is a format that summarizes information of a patient.
If you improve this step further, remember that it’s important to make a “Suggestion” with assessment sheet.
To prevent people from looking at the assessment sheet from thinking, “So what will happen next ?” proposal is needed what we have to do next.
If you can do this, you will be recognized as excellent nurse at work.
At this time, you’ll have to use “SBAR” too, specially emergency case.
SBAR is from the initials of “S: Situation”, “B: Background”, “A: Assessment”, and “R: Recommendation”.
We always consider and are able to communicate quickly and appropriately.
In particular, there are more situations where SBAR is used for urgent requirements, so let’s keep the main points in mind when reporting.
When conducting an assessment, if your assessment has a suggestions too, it will be easier for the others who listen to you to understand your conclusion.
Case Study with SBAR

Let’s understand the Case Study by using SBAR.
Patient with stomachache
This is one case study with a patient with stomachache.
Let’s see the conversation between the nurse and the doctor by using SBAR.
【S: Situation】
The patient 30 years old, male is telling me a serious stomachache.
OK ! What’s next ?
【B: Background】
He had a rice, soup and grilled fish for dinner yesterday.
And he had history of myocardial infarction.
I see.
【A: Assessment】
He still has conscious. Blood pressure is 150/90, body temperature is 36.5 ℃, pulse is 80 and 15 breaths.
【R: Recommendation】
Could you see him immediately ?
Understood. I will visit soon.
In this case, the patient suddenly complained of abdominal pain, but the nurse was able to quickly tell the doctor what the doctor wanted to know according to SBAR.
In most cases, you report to doctor by phone, but try not to ask the doctor.
As a bad example, Take care of not to be asked many times by the doctor “How is blood pressure?”, “Umm, I will check it” “What about breaths ?”, “I will check it.”.
Doctor is very busy, so you try to anticipate questions in advance and gather information before contacting the doctor.
Patient with fever
Next case study is a patient with fever.
Let’s see how the nurse uses SBAR too.
【S: Situation】
The patient 28 years old, female has a fever of 38.5 ℃
OK ! What’s next ?
【B: Background】
She seems to have been feeling unwell for 2 hours, but she has a urinary catheter, so a urinary tract infection is suspected.
【A: Assessment】
Respiration is 25, pulse is 90, *SpO2 is 96%, and there is no adventitious lung noise.
*SpO2: Oxygen Saturation Percutaneous
I see.
【R: Recommendation】
Could you come to patient’s home immediately ?
OK. Please wait for 15 minutes.
In this case, SBAR was successfully used, and the necessary information and requests to the doctor were quickly told with minimal communication.
Ultimately, what you want to ask the doctor is “Please visit here immediately.”. But do not ask the doctor like that soon.
Because the doctor has a lack of critical information yet as to why he is necessary to go right now.
In this way, a certain amount of experience and tricks are required to use SBAR.
So that, you can quickly tell what you want to say, let’s always be conscious and work on it.
I can imagine that situation to use SBAR is not in Japan only but it’s also other country.
I hope you successfully utilize SBAR in your any Home Nursing Station and Hospital too.
Conclusion

I explained the overview of the assessment and how to use the assessment sheet.
Again, the assessment sheet is a means, not our goal.
The primary purpose of using assessment sheets is to provide appropriate care and services to patients.
Assessment sheets exist so that medical professionals can make appropriate decisions based on correct information.
I also explained that “SBAR” is important in emergency cases.
I hope you become a good nurse standing by all patients.

